
What Will Health Care Look like in 20-Years?
The Microbiome: Beyond the Gut
The Microbiome/Inflammation/Infection Link
The Microbiome/Environment Link
Genomics: The Revolution We’ve All Been Waiting For
Pharmacogenomics
Medicine Goes Mobile
Immunotherapy … and more
Courtesy Medscape
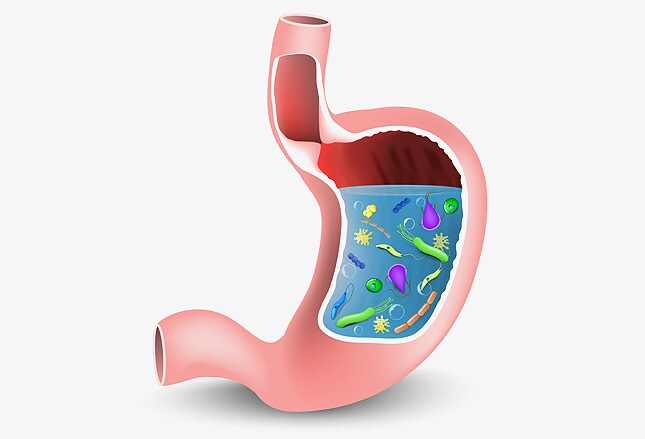
The Microbiome: Beyond the Gut
Understanding of the world beneath—the seething, teeming microbial world that inhabits every orifice and surface of the body—has led to a whole new paradigm in the prevention and treatment of a range of diseases. Studies examining the gut microbiome led to an explosion of research that linked disruptions in the microbiota to conditions from atopy to cardiovascular disease. David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School in Norfolk, predicts that over the next 20 years, the “gut microbiome effect on health and disease will become clearer. Identification of microbial dysbiosis and directed efforts to restore more normative equilibrium in microflora will transform our current approach to disease management—for gastrointestinal disease and beyond.”
The Microbiome/Inflammation/Infection Link
Back in the day—pre-2000—a patient with a cough was categorized as having an infectious process or an inflammatory (ie, allergic) process. No longer. Disruptions in the microbiome are now recognized to play a pivotal role in the development of acute and chronic processes. The “microbiota hypothesis”[1] proposes that alterations in the microbiome disrupt host homeostasis and, therefore, affect disease risk in myriad ways, with manifestations ranging from alterations in immunity to changes in metabolism.
Recognizing, and learning to minimize, the many factors that can disrupt the microbiome will continue to be a focus of research. Antibiotics may be the best known of these disruptors, but numerous other environmental factors, including changes in population density, proximity to animals, pollution, and diet, are all now known to effect the transmission and maintenance of indigenous microbiota.
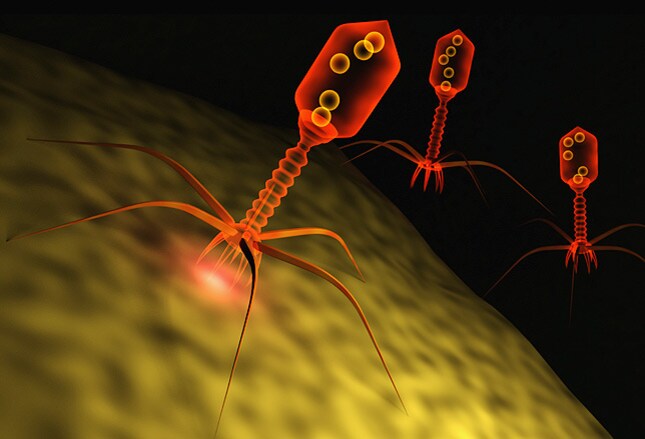
A Medscape reader predicted that the next two decades would bring a better “understanding of how and why microbes cause chronic inflammatory disease.” Hand in hand with this improved understanding of the microbiome and its important role in maintaining health will be increased therapeutic use of bacteriophages, already widely used in agriculture,[1] that only minimally disrupt normal flora[2] in order to treat infections caused by resistant organisms.
Image from Dreamstime
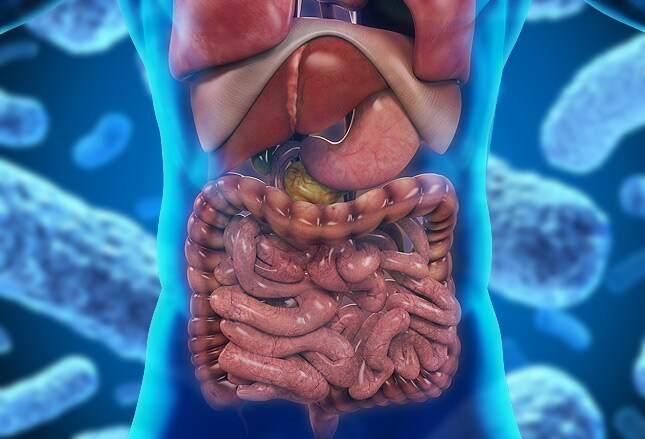
The Microbiome/Chronic Disease Link
It is recognized that microbiota composition is altered in patients with various chronic inflammatory conditions. In addition to gastrointestinal conditions, such as Crohn disease,[3] ulcerative colitis,[4] and irritable bowel syndrome,[5] dysbiosis, or microbial imbalance, has been associated with psoriasis,[6]both type 1[7] and type 2[8] diabetes, and cardiovascular disease.[9] Dr Johnson commented that the emerging evidence strongly suggests that changes in the gut microbiota play a pivotal role in the regulation of energy homeostasis and the development and progression of obesity and its associated metabolic disorders. Myron Genel, MD, professor emeritus of pediatrics and senior research scientist at Yale Child Health Research Center, speculated that potential therapeutic interventions would be developed “on the basis of a better understanding of the pathophysiologic implications of microflora in body cavities.” Dr Johnson added that although it appears that manipulation of the gut flora may be an avenue for potential new targeted therapies, further studies are necessary before introducing them into standard clinical practice. The hope is that this enhanced understanding will finally begin to yield results that will improve the management of chronic disorders, autoimmune disease, allergy, and even dental disease in the decades to come.

The Microbiome/Environment Link
It is now well-known that microbial equilibrium can be disrupted by antibiotics, probiotics, dietary factors, environmental contaminants, and even stress. Will the next 20 years bring therapies that intentionally alter microbiota to produce a desired effect, similar to today’s use of fecal transplantation in the treatment of recurrent Clostridium difficile infection? Will knowledge of an individual’s microbiota profile become essential in tailoring therapy? The American Gut Project, by encouraging the general public to participate, seeks to create a robust and comprehensive reference set of microbiome samples and metadata available for unrestricted use by researchers. The goal of the project is to improve understanding of population-wide variances and enable stringent hypothesis testing and evaluation of effect sizes.[10] Although none of our experts were willing to hazard a guess about specific therapies or developments that will result from this widening investigation of the microbiome, all were certain that it would result in insights that will definitively alter the way we prevent and treat a wide spectrum of disease.
Genomics: The Revolution We’ve All Been Waiting For
On April 14, 2003, the International Human Genome Sequencing Consortium announced the successful completion of the Human Genome Project.[11] Predictions of its impact on health and amelioration of disease proliferated…and in many cases fizzled. Yet slowly but surely, one painstaking study after another, the collective science community added new insights to our understanding of the human genome and the potential for gene therapy to revolutionize the care of patients across a wide spectrum of disease as well as prevent disease in successive generations. What are some of the specific ways in which advances in understanding of genomics might change medicine?

Understanding Disease
Exome and genome sequencing have allowed identification of the genetic causes of neurologic disease and potentially the ability to prevent or mitigate these disorders, but the hope in the future is that these will also extend to a wide array of diseases. Maurie Markman, MD, a clinical professor at Drexel University College of Medicine and president, Medical & Science, at the Cancer Treatment Centers of America in Philadelphia, notes that an improved knowledge of germline data is already an important area of cancer risk (eg, BRCA mutations). Eric Topol, MD, Medscape’s editor-in-chief, enthuses that “we are indeed in the midst of a genomic revolution, with CRISPR genome editing moving into clinical trials for the detection and treatment of cancer and infectious disease, fetal screening for chromosomal abnormalities, and molecular diagnosis of unknown diseases. This will accelerate: Whereas 1 million humans have had genome sequencing in 2015, the projection is that more than 1 billion people will have been sequenced by 2025.” William F. Balistreri, MD, professor at Cincinnati Children’s Hospital Medical Center, looks forward to the potential of whole-exome sequencing to assist in accurately diagnosing diseases and in structuring personalized medicine. “Whole-exome sequencing offers a high yield of relevant predictive and diagnostic information, which will be used in the evaluation of patients with suspected genetic disorders. The diagnostic success resulting from exome sequencing will lead to the development of novel, targeted treatment strategies.”
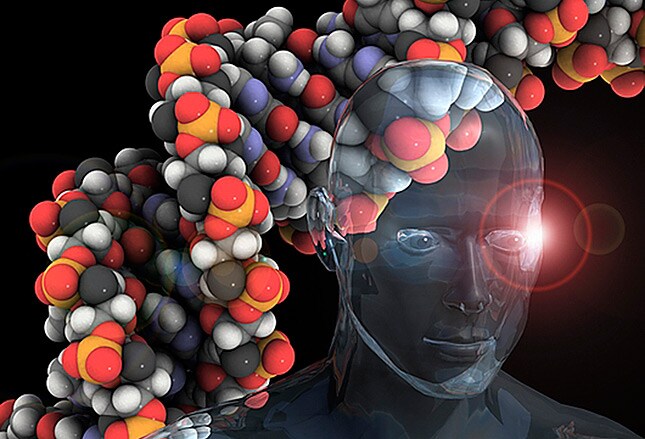
Along these same lines, John G. Bartlett, MD, professor emeritus in the Department of Medicine at Johns Hopkins Hospital in Baltimore, Maryland, predicts that gene sequencing will become routine and serve as the “standard for infection control, epidemic control, and food safety.” William T. Basco, MD, MS, professor of pediatrics and director, Division of General Pediatrics at the Medical University of South Carolina, is enthused about the potential for the increased availability of genomic data to help predict individual response to therapeutics, including in autoimmune conditions, but perhaps also for other prevalent conditions, such as asthma, attention-deficit/hyperactivity disorder, and seizure disorders. “Wouldn’t it be nice to know which drug a patient is more likely to respond to rather than just taking a guess?”
Image from Science Photo Library

Pharmacogenomics
Drugs are currently “one size fits all”—but pharmacogenomics is changing that, by looking at how our genes affect our response to drugs. Experts such as the Clinical Pharmacogenetics Implementation Consortium anticipate that a growing knowledge and understanding of germline genomic data will be translated into actionable guidelines for use of an array of drugs that will lead to widespread use of pre-prescription genotyping.
Although still in its infancy, the hope moving forward is that pharmacogenomics will allow patient-tailored therapy for a wide range of diseases. Of course, the barriers to its use will include cost, because these therapies can be anticipated to be monumentally expensive.

Pharmacogenomics in Cancer
Nearly every aspect of cancer research has benefited from The Cancer Genome Atlas[12], according to Bert Vogelstein, MD, Clayton Professor of Oncology and Pathology at the Sidney Kimmel Comprehensive Cancer Center at Johns Hopkins University. Begun in 2006 and completed in 2015, the Atlas is a compilation of the genomic changes in all cancers and is a “source book” informing the practice of individualized cancer therapy. Gene sequencing of specific tumors has allowed identification of precision therapies to treat cancers, regardless of where in the body they may occur. In 20 years, the division of cancers into brain or breast or prostate will be eliminated. The improved understanding of the normal germline as well as genetic mutations in individual tumors will allow specialists in tumor type to aggregate information and develop strategies to treat patients with specifically targeted therapies. In addition to better knowledge of cancer genomes, advances in the understanding of the normal human germline and its variations will allow clinicians to predict differences in the ability of an individual to metabolize a chemotherapeutic agent (or other drugs).

Immunotherapy
The progress over the past year in the development of a significant number of new immunotherapies for the treatment of cancer has been unprecedented. From new data supporting use of atezolizumabfor the treatment of non-small cell lung cancer to the US Food and Drug Administration’s approval ofnivolumab for treatment of renal cell carcinoma, cancer experts have cheered the mounting evidence of long-term efficacy and clinical benefit in rare cancers. A dramatic example of the potential for this group of therapies came in December 2015 with the announcement by former president Jimmy Carter that he no longer has evidence of active cancer in his brain after treatment with a recently approved immunotherapy for melanoma that had metastasized to his brain. Dr Markman predicts that this is just the start and that over the next two decades, “the single most important goal/innovation will be the development of a complete understanding of how to establish a highly effective anticancer immune response in individual patients that will successfully control the growth and spread of their cancer. This will include activation or reversal of suppression of the response, as well as prevention of an excessive response that results in unacceptable toxicity.”
Although immunotherapy has been most investigated as a cancer therapy, research can be expected in other disease states, such as autoimmune disorders. As with genomic therapies, however, potential barriers, such as huge cost, will have to be overcome before treatment will be widely implemented.

Business of Medicine
The whole paradigm of healthcare is shifting, and will continue to shift—from technological advances (finally, an electronic health record that works!) to changes in the historic doctor/patient relationship (patient empowerment) and changes in the way in which healthcare is financed (with creation of ever-larger healthcare conglomerates). These changes will go well beyond the upheaval begun with the Affordable Care Act’s passage in 2010.
Medicine Goes Mobile
Robert Glatter, MD, editor-at-large for Medscape Emergency Medicine, assistant professor at Hofstra North Shore-LIJ School of Medicine, and an attending physician in emergency medicine at Lenox Hill Hospital in New York, predicts that one of the “most significant breakthroughs in the practice of emergency medicine will be the routine use of the smartphone for gathering patient data and integrating it into triage and assessment” and also for making laboratory and imaging data available at the point of care. Handheld point-of-care ultrasound (in a smartphone or tablet) will likely replace the stethoscope and other routine aspects of the physical examination of patients. Emerging 3D and 4D ultrasound technology will become a cornerstone of medical education and a requisite aspect in the care of patients.
The smartphone will be part of not only patient assessment but also the diagnostic process, through the use of mobile algorithms, and management, including the ever-widening use of e-prescribing.
Immunotherapy
The progress over the past year in the development of a significant number of new immunotherapies for the treatment of cancer has been unprecedented. From new data supporting use of atezolizumabfor the treatment of non-small cell lung cancer to the US Food and Drug Administration’s approval ofnivolumab for treatment of renal cell carcinoma, cancer experts have cheered the mounting evidence of long-term efficacy and clinical benefit in rare cancers. A dramatic example of the potential for this group of therapies came in December 2015 with the announcement by former president Jimmy Carter that he no longer has evidence of active cancer in his brain after treatment with a recently approved immunotherapy for melanoma that had metastasized to his brain. Dr Markman predicts that this is just the start and that over the next two decades, “the single most important goal/innovation will be the development of a complete understanding of how to establish a highly effective anticancer immune response in individual patients that will successfully control the growth and spread of their cancer. This will include activation or reversal of suppression of the response, as well as prevention of an excessive response that results in unacceptable toxicity.”
Although immunotherapy has been most investigated as a cancer therapy, research can be expected in other disease states, such as autoimmune disorders. As with genomic therapies, however, potential barriers, such as huge cost, will have to be overcome before treatment will be widely implemented.
Image from Mark Humphrey/AP
The Rise of the Patient
Dr Topol has long advocated for the empowered patient, most notably in his book The Patient Will See You Now, which anticipates smartphone-based apps that will allow patients to view their own lab results, monitor vital signs, and apply artificially intelligent algorithms to diagnose themselves. Desiree Lie, MD, a clinical professor in the Department of Family Medicine at the Keck School of Medicine at the University of Southern California in Los Angeles, envisions online electronic portals that will provide access to the individual’s current health status, suggest behavior changes, calculate current and ideal body mass index, set blood pressure targets, offer needed advice about lifestyle changes, and notify patients when preventive care is needed. These resources will calculate a “health report card” that will coach users on how to attain the best health outcomes. “It would be like having a bank statement of one’s health or a financial retirement projection to help the consumer achieve the best long-term outcome.” Valerie Gilchrist, MD, professor and chair of the Department of Family Medicine at the University of Wisconsin in Madison, likens it to a personal electronic medical record. Greater patient control will translate to more emphasis on wellness and patient accountability for their health, predicts Renee S. Holleran, RN, PhD, a nurse at Intermountain Medical Center in Salt Lake City, Utah.


Leave A Comment